
By Dr Jonathan Shurlock
Edited by Dr Nitin Chandra Mohan
The results of the DanGer Shock trial were recently presented at the American College of Cardiology congress alongside a simultaneous publication in the New England Journal of Medicine. The results, presented by Professor Jacob Møller have resulted in broad discussion regarding mechanical circulatory support for patients suffering with ST-segment elevation myocardial infarction complicated by cardiogenic shock.
Briefly, this multi-centre trial, randomised 360 patients with STEMI to either standard care plus Impella placement (n=179), versus standard care alone (n=176). The primary outcome measure was all cause mortality at 180 days. Death from any cause occurred in 82 of 179 in the Impella group, versus 103 of 176 in the control group (hazard ratio, 0.74; 95% confidence interval [CI], 0.55 to 0.99; P=0.04). Secondary composite safety endpoint of severe bleeding, limb ischaemia, device failure, haemolysis, and worsening aortic regurgitation was higher in the Impella group (24% vs 6.2%; relative risk [RR] 4.74; 95% CI 2.36-9.55)in addition to an increased requirement for renal replacement therapy.
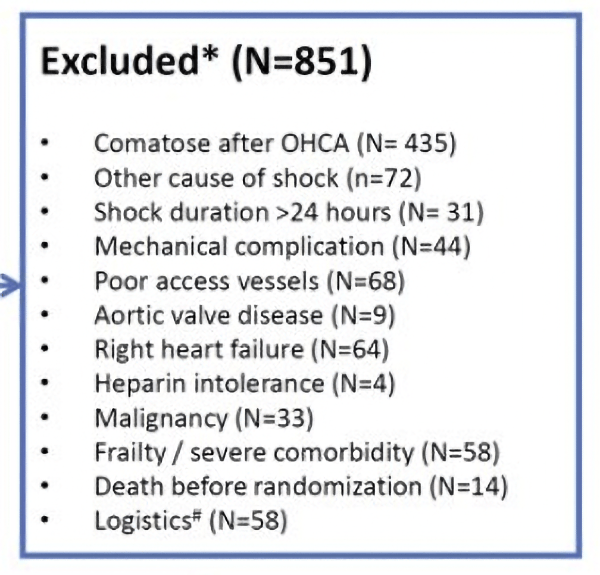
The persistence of the research team is commendable, with trial enrolment taking a decade. Professor Møller highlighted the need to be cautious in wider extrapolation of the results for causes of cardiogenic shock other than STEMI. Sub-group analysis showed an overall benefit in males with a signal for harm in female patients. There further appeared to be greater benefit in patients presenting with MAP <63mmHg. When considering these results and their applicability to broader clinical practice, clinicians should consider the trials exclusion criteria (See below).
This is the first adequately powered study to show benefits of routine use of Impella in a select group of patients. However, the rate of adverse safety events in the Impella arm with a number needed to harm of 6 is concerning. There also remains lack of clarity on timing of pump placement, how various types of mechanical circulatory support may be combined and how it might be implemented in local shock protocols. Furthermore, the question remains how the device would perform in unselected centres in a more heterogeneous group of patients with cardiogenic shock.
See the full trial here: https://www.nejm.org/doi/full/10.1056/NEJMoa2312572